
Sponsored by EssilorLuxotica
New research on myopia progression control technologies has shown promising long-term efficacy. Is it time to rethink current treatment and clinical trial paradigms?
The global prevalence of myopia continues to rise, driving researchers, clinicians and industry stakeholders to explore new strategies for its management. At the annual meeting of The Association for Research in Vision and Ophthalmology (ARVO 2025), EssilorLuxottica (France) demonstrated how it is addressing this growing challenge head-on— advancing the standard of care for children with myopia worldwide.
At an EssilorLuxottica-sponsored event on Day 2, experts Prof. Mark Bullimore of the University of Houston College of Optometry and Dr. Norbert Gorny, Chief Scientific Officer at EssilorLuxottica, presented the latest research on myopia and myopia management mechanisms, while highlighting current challenges in the field and opportunities to enhance understanding through research and collaboration.
READ MORE: The Myopia Enigma
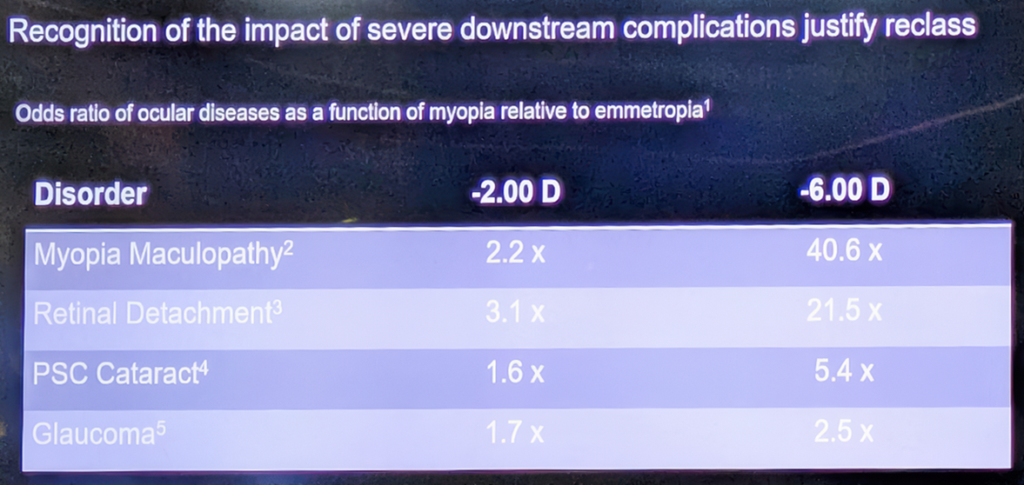
Dr. Gorny discussed how current classifications of myopia may influence how the condition is addressed in both clinical and regulatory settings. He suggested that reframing myopia as a condition with long-term health implications could help inform the development, evaluation and regulation of interventions. He referenced research demonstrating that individuals with higher degrees of myopia face an increased risk of several sight-threatening conditions, including myopic maculopathies, retinal detachment and early-onset glaucoma. This view aligns with a broader movement in the vision science community advocating for more comprehensive and early-stage intervention strategies, which may include environmental, behavioral, optical and pharmacological measures.
What are these approaches to managing myopia? What does the research and clinical evidence reveal about their effectiveness and underlying mechanisms? And importantly—what comes next?
READ MORE: Experts Discuss Strategies and Creative Approaches in Myopia Management
Cellular mechanisms and long-term efficacy data for lenses that slow myopia progression
Recent advances in understanding the cellular mechanisms behind myopia development have become foundational to our evolving understanding of myopia and how to treat it. Dr. Gorny shared preclinical data using animal models to explore how the retina processes defocus signals—work that may inform future device designs. While the clinical relevance of this mechanism continues to be evaluated, such studies represent one part of a multi-faceted research effort.
“We have identified a certain type of retinal ganglion cell that is sensitive to the processing of defocus signals,” Dr. Gorny explained. “This cell type showed a very significant and characteristic firing pattern when exposed to a myopic defocus.”
Specifically, the research revealed that efficacious myopia progression control spectacle lenses produce distinctive patterns on the retina characterized by changes in local spatial contrast, potentially triggering the mechanism for slowing axial length growth.
While the precise mechanisms continue to be explored, understanding the long-term impact of these interventions is critical. Six-year clinical data from EssilorLuxottica demonstrated that Essilor® Stellest® lenses slowed down myopia progression by 1.95 D (57%) and slowed axial elongation by 0.81 mm (52%) on average, compared to an extrapolated single-vision lens control group model based on data from the first two years of the clinical trial.1
Importantly, no evidence suggesting a rebound effect in myopia progression has been observed following discontinuation of Essilor® Stellest® lens wear2—an outcome that has been reported with some other interventions.
Navigating regulatory pathways and evolving clinical trial designs
Dr. Gorny’s revelation of new underlying structural disease mechanisms and the latest clinical data argue strongly in favor of using myopia progression control lenses like EssilorLuxottica’s Essilor® Stellest® lenses. So why aren’t these technologies finding their way in front of the pediatric eyes that need them so urgently?
Both Dr. Gorny and Prof. Bullimore acknowledged the high-level rigorous processes required to have solutions vetted through the regulatory pathways for myopia progression control technologies. Currently, only a limited number of interventions—such as specific soft contact lenses and overnight orthokeratology—have received FDA approval for managing myopia progression in children.
Dr. Gorny also reflected on how the current regulatory endpoints could better align with recent advancements in research and evolving clinical practices. He suggested that treatment evaluations could potentially benefit from a more tailored approach, taking into account not only efficacy, but also factors such as the type of intervention, its risk profile, accessibility, affordability and broader public health implications.
The next step for clinical trials
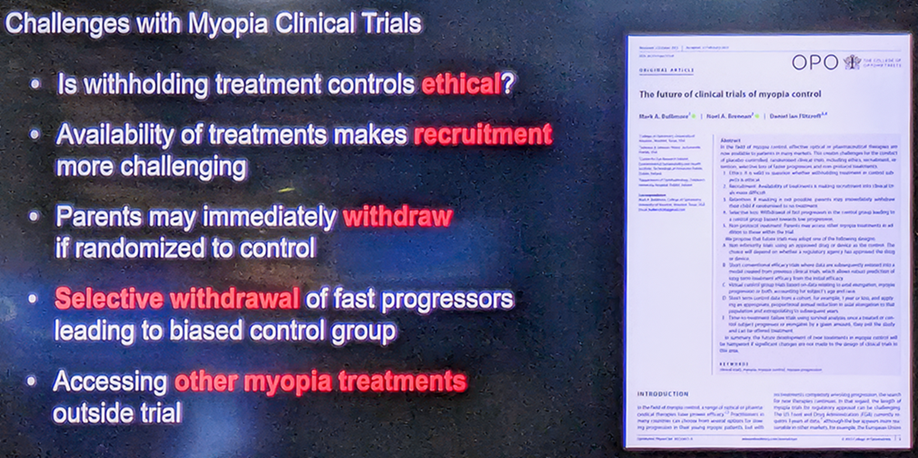
Prof. Bullimore’s presentation focused on developing clinical trial approaches for myopia progression control, to overcome obstacles to bringing interventions to market in a timely manner.
He highlighted the ethical and practical challenges of enrolling children in long-term control groups, which could delay the availability of effective interventions. “Is it really ethical, given what we know about myopia and the increased risk of uncorrectable vision impairment, to withhold treatment for a child for 2 or 3 years?” he asked.
“He noted that traditional randomized clinical trial models may present logistical and ethical challenges, particularly in recruiting pediatric participants for control groups, even in shorter-duration studies.”
He outlined several alternative approaches that could speed up time to market.3,4 One such model he proposed involves clinical trial designs that integrate shorter randomized periods combined with predictive modeling to project long-term outcomes.
“Where we could end up is some sort of hybrid approach, where you randomize kids for one year, estimate the one-year efficacy and use that to predict what the three-year efficacy might be, and even the six-year efficacy,” Prof. Bullimore said.
Another model explored involved allowing participants to exit clinical trials once they reach a predetermined progression threshold, offering a potential solution to accelerate trials while ensuring ethical standards are met.
Reassessing safety and advancing collaborative solutions
Prof. Bullimore concluded by highlighting some important considerations in the evolving landscape of myopia progression control interventions, including safety and potential rebound effects after treatment cessation.
He began with rebound, indicating the need for a perspective shift on how to assess it. “Rebound cannot be assessed by comparing progression after treatment with progression during treatment,” he said. “It can only be assessed by comparing progression after treatment with progression in untreated patients.”
For myopia progression control lenses like Essilor® Stellest® lenses, Prof. Bullimore presented evidence that, while rebound exists for certain interventions like red light therapy and higher concentrations of atropine, “no rebound effect has been observed for optical interventions—and we don’t need to burden children or sponsors with additional evaluations after treatment.”5
READ MORE: The Atropine Conundrum: Decoding Conflicting Research Results
Safety considerations were also discussed in the context of various interventions, with proportionate risk assessment based on the specific technology being evaluated. With concerns rising about potential retinal damage from red light therapy, Prof. Bullimore noted the comparative safety profile of a device like myopia progression control lenses.
“In the case of the Essilor® Stellest® lens, every aspect of vision you can think of has been measured in children and adults wearing this lens,” he said. This data reinforces the lenses’ favorable safety profile compared to other myopia management interventions.6-9
As Prof. Bullimore wrapped up his presentation, he called for a broader, more collaborative approach to addressing myopia as a public health issue. He raised the question of whether the current regulatory and clinical trial systems are sufficiently adaptive to support the timely evaluation and availability of innovations, particularly in light of the rising global prevalence of myopia.
“There is some interest in getting some brains together to think about these issues,” he said, pointing to the power of collaboration under organizations like the International Myopia Institute. “If we believe myopia to be a public health problem, how can we justify conducting clinical trials and continuing business as usual in the same way in which we’ve been asked to do it?”
The session concluded with Dr. Gorny stating the great benefit that timely action can offer to the millions of myopic individuals worldwide at risk of progression and associated ocular complications, including potential visual impairment. “Every diopter matters. And we need to accelerate our efforts to bring these products everywhere into clinical and practical use because we’re losing time. And by losing time, we’re losing opportunities for the children that are awaiting treatment.”
READ MORE: Stay on top of ARVO 2025—find expert insights and daily highlights here.
Editor’s Note: Reporting for this story took place during the annual meeting of The Association for Research in Vision and Ophthalmology (ARVO 2025) being held from 4-8 May in Salt Lake City, Utah, United States.
References
- EssilorLuxottica. Myopia control efficacy of spectacle lenses with highly aspherical lenslets: results of a 6-year follow-up study. 2025. Data on file.
- Sankaridurg P, Weng R, Tran H, et al. Spectacle Lenses With Highly Aspherical Lenslets for Slowing Myopia: A Randomized, Double-Blind, Cross-Over Clinical Trial: Parts of these data were presented as a poster at the Annual Research in Vision and Ophthalmology meeting, 2022. Am J Ophthalmol. 2023;247:18-24.
- Bullimore MA, Brennan NA, Flitcroft DI. The future of clinical trials of myopia control. Ophthalmic Physiol Opt 2023;43:525-33.
- Brennan NA, Shamp W, Maynes E, et al. Influence of age and race on axial elongation in myopic children: A systematic review and meta-regression. Optom Vis Sci 2024;101:497-507.
- Bullimore MA, Brennan NA. Efficacy in myopia control-The impact of rebound. Ophthalmic Physiol Opt. 2025;45(1):100-110.
- Gao Y, Lim EW, Yang A, Drobe B, Bullimore MA. The impact of spectacle lenses for myopia control on visual functions. Ophthalmic Physiol Opt. 2021;41(6):1320-1331.
- Huang Y, Li X, Wang C, Zhou F, Yang A, Chen H, Bao J. Visual acuity, near phoria and accommodation in myopic children using spectacle lenses with aspherical lenslets: results from a randomized clinical trial. Eye Vis (Lond). 2022;9(1):33.
- Gao Y, Spiegel DP, Muzahid IAI, Lim EW, Drobe B. Spectacles with highly aspherical lenslets for myopia control do not change visual sensitivity in automated static perimetry. Front Neurosci. 2022;16:996908.
- Gao Y, Lim EW, Drobe B. Impact of myopia control spectacle lenses with highly aspherical lenslets on peripheral visual acuity and central visual acuity with peripheral gaze. Ophthalmic Physiol Opt. 2023;43(3):566-571.


